Semaglutide Before and After 30 Days Results
Medical Reviewer: Arthur L Burnett, MD
Table of Contents
- 1. How Semaglutide Works in the First 30 Days
- 2. The 0.25 mg Starting Dose and Titration Schedule
- 3. What Clinical Trials Say About Month One Benchmarks
- 4. Analyzing Visual Transformations and Body Composition Changes
- 5. Critical Biological Factors Influencing Early Weight Loss Outcomes
- 6. Managing First-Month Side Effects and Gastrointestinal Dynamics
- 7. Product Selection and Standard Administration Guidelines
- 8. Optimal Nutrition and Lifestyle Frameworks for Early Success
- 9. Comparing Metrics: Type 2 Diabetes vs. Non-Diabetic Patients
- 10. Navigating Beyond Day 30: Progressing Your Maintenance Protocol
- 11. Comprehensive Frequently Asked Questions (FAQs)
1. How Semaglutide Works in the First 30 Days
Embarking on a metabolic restoration protocol requires an evidence-based perspective on what happens inside your body during the initial weeks. When analyzing your expected Semaglutide Before and After 30 Days Results, it is crucial to recognize that the drug functions as a structural analog to native glucagon-like peptide-1 (GLP-1). This endogenous incretin hormone is typically secreted by the L-cells of your lower part of the intestine in response to nutritional intake. According to metabolic research archives available on the National Institutes of Health (NIH) Portal, this synthetic peptide is highly resistant to rapid enzyme degradation compared to your body’s natural hormones.
During the early phase of therapy, the compound slowly accumulates in the bloodstream to initiate your first 4 weeks progress. It operates primarily through three distinct organ-system pathways:
- Central Nervous System Modulation: The molecule successfully navigates across the blood-brain barrier, directly binding to specific arcuate nucleus receptors within your hypothalamus to downregulate baseline hunger signals and eliminate persistent, intrusive food noise.
- Slower Digestion (ખોરાક ધીમેથી પચવો): It actively reduces gastric smooth muscle contractility. This creates slower digestion, meaning ingested food remains inside the stomach cavity for a significantly prolonged duration to sustain physical fullness.
- Pancreatic Endocrine Optimization: It enhances glucose-dependent insulin expression from your beta cells while simultaneously blunting excessive glucagon release from alpha cells, establishing tight glycemic control.
Because the half-life of this modified peptide is roughly 168 hours, your body requires nearly five continuous weeks of consistent weekly dosing to establish a stable physiological concentration. Therefore, your first month acts as a biological onboarding phase designed to condition your peripheral metabolic receptors rather than to maximize fat-burning capacity.
2. The 0.25 mg Starting Dose and Titration Schedule
A frequent error among patients tracking their early weight management timeline is expecting maximum clinical efficacy immediately at day one. To safeguard gastrointestinal health and ensure long-term clinical compliance, medical protocols follow a strict, incremental step-up schedule reviewed and regulated under the U.S. Food and Drug Administration (FDA) Safety Standards. Your initial 30 days updates are achieved entirely while taking a foundational introductory dose of 0.25 mg subcutaneously once per week.
Clinical Review Note from Dr. Arthur L Burnett: “The target of the initial 0.25 mg step during the first 30 days is not to drop massive amounts of adipose tissue. The true therapeutic goal is to allow your enteric nervous system and digestive tracking pathways to safely adapt to altered motility speeds without triggering severe adverse reactions.”
Bypassing this onboarding phase or prematurely escalating your dosage increases the risk of severe acute side effects, such as intractable vomiting, profound abdominal cramping, and secondary dehydration that may require clinical intervention. Patience during these first 4 weeks creates the physiological groundwork for the accelerated fat loss that typically presents during subsequent titration steps.
3. What Clinical Trials Say About Month One Benchmarks
Data compiled from double-blind, placebo-controlled clinical investigations—most notably the global STEP (Semaglutide Treatment Effect in People with Obesity) research initiatives published in the NIH National Medicine Registry—provide clear parameters regarding what baseline metrics look like. Clinical cohorts indicate that standard, healthy progress yields an initial weight loss of 2% to 4% of total baseline body weight over the first 4 weeks.
To evaluate these statistics across diverse body masses, examine the standard clinical expectations outlined in the tracking matrix below:
| Baseline Starting Weight | Average 2% Mass Reduction (Day 30) | Average 4% Mass Reduction (Day 30) |
|---|---|---|
| 200 lbs (90.7 kg) | 4.0 lbs (1.8 kg) | 8.0 lbs (3.6 kg) |
| 250 lbs (113.4 kg) | 5.0 lbs (2.3 kg) | 10.0 lbs (4.5 kg) |
| 300 lbs (136.0 kg) | 6.0 lbs (2.7 kg) | 12.0 lbs (5.4 kg) |
It is clinically valuable to note that this initial mass reduction does not consist entirely of pure adipose tissue catabolism. Instead, early scale drops reflect a substantial decrease in chronic, systemic water retention alongside a reduction in visceral tissue inflammation, paired with an average 24% voluntary reduction in baseline caloric intake due to early appetite changes.
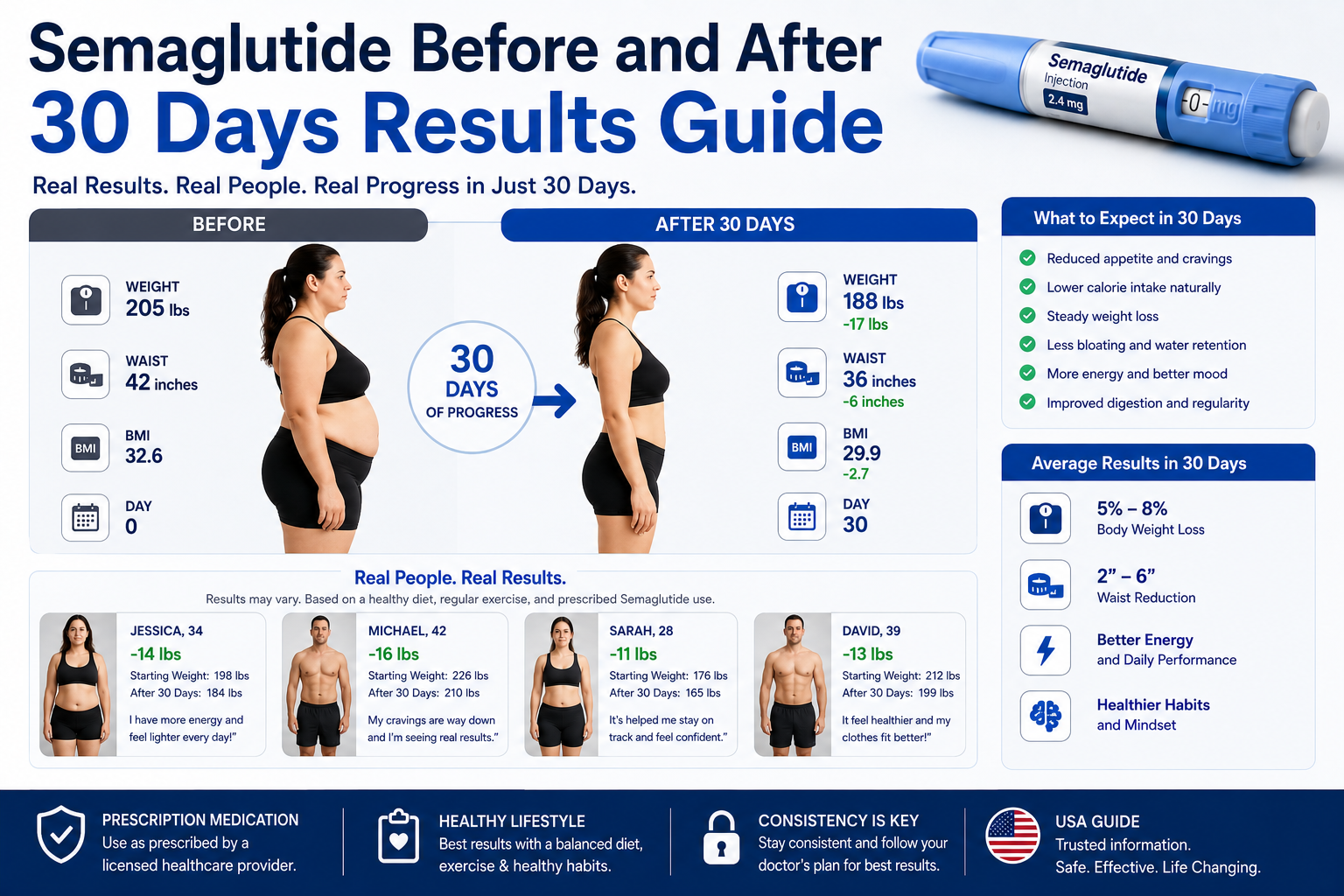
4. Analyzing Visual Transformations and Body Composition Changes
When searching for real-world visual examples of an initial weight loss changes timeline or tracking early updates, it is critical to balance visual expectations with physiological facts. Because medical safety guidelines prioritize a steady drop of 1 to 2 pounds per week, drastic changes in body shape are rarely visible in a 30-day mirror comparison. Instead, early progress presents as structural and systemic updates.
The standard visual and physical adaptations reported at the 30-day mark include:
- Systemic Fluid De-puffing: Substantial drops in superficial facial edema, periorbital puffiness, and lower abdominal distension as systemic inflammatory pathways clear out.
- Altered Micro-Measurements: Small shifts in how clothing fits around your waist, midsection, and neck, allowing structured garments to sit more comfortably even if the numerical scale movement appears modest.
- Postural and Mechanical Relief: Noticeable reductions in minor joint stress and morning mobility issues, driven by the elimination of the first few pounds of excess systemic weight.
5. Critical Biological Factors Influencing Early Weight Loss Outcomes
Every individual exhibits a highly personalized metabolic signature, meaning that your personal Semaglutide Before and After 30 Days Results may deviate from generalized averages. Several key biological variables directly dictate the rate and depth of your early month-one progress:
Baseline Metabolic Flexibility and Age
Younger demographics or individuals with higher levels of residual lean muscle mass typically show immediate responses to initial GLP-1 receptor activation. Conversely, individuals navigating long-standing metabolic syndrome or severe insulin resistance often experience a slower start as their cellular pathways adjust.
Genetic Incretin Receptor Receptivity
Variations in your genetic GLP-1 receptor expression mean some individuals function as extreme early responders, noting profound appetite changes on the minimal 0.25 mg introductory dose. Others require higher doses before experiencing the same level of receptor saturation.
6. Managing First-Month Side Effects and Gastrointestinal Dynamics
As your digestive architecture learns to manage delayed stomach emptying, minor to moderate side effects may surface. These changes are typically benign and self-limiting, resolving as your tissues build metabolic tolerance to the peptide.
The most common issues encountered during the initial 30 days of therapy include:
- Transient Nausea: Frequently presenting when you consume meals too rapidly or choose items rich in saturated fats.
- Altered Bowel Motility (Constipation): A direct byproduct of slower digestion across your intestinal tract, requiring proactive hydration protocols.
- Gastric Acid Reflux: Food remaining in the stomach chamber longer can elevate upward pressure on the lower esophageal sphincter.
- Mild Secondary Fatigue: Usually a direct physiological response to a sudden, rapid drop in daily caloric intake rather than a toxic reaction to the medication.
7. Product Selection and Standard Administration Guidelines
Achieving stable weight drops depends heavily on sourcing authenticated medication and using correct medical protocols. For a complete analysis of your long-term treatment path, consult the foundational Semaglutide Weight Loss Timeline Guide to ensure your long-term titration remains mathematically sound.
To guarantee safety and continuous clinical supervision throughout your first month, explore the options available in our dedicated Semaglutide Weight Loss Program, which provides verified pharmaceutical formulations and medical guidance.
Available Treatment Options & Sourcing
Depending on your customized treatment plan, your provider will typically prescribe balanced choices to maximize your initial weight loss changes:
- Injectable Formulations (Starter Pack): For individuals beginning their weekly subcutaneous titration, you can browse options directly through the official online store’s Semaglutide Injection Collection, optimized specifically for month-one gastrointestinal onboarding.
- Oral Tablet Alternatives: For patients seeking a non-injectable routine, the complete Rybelsus Semaglutide Oral Tablets Collection provides daily oral support.
8. Optimal Nutrition and Lifestyle Frameworks for Early Success
Semaglutide is an exceptionally effective medical tool, but its clinical impact relies heavily on concurrent lifestyle alignment. To optimize your early 30-day outcomes and protect your metabolic rate, implement these clinical strategies:
Prioritize Lean Amino Acid Intake
Because overall food intake drops significantly, your daily protein intake must be actively managed to protect against lean muscle tissue wasting. Center your meals around skinless poultry, egg whites, and low-fat Greek yogurt.
Maintain Strict Fluid and Electrolyte Tracking
Slower digestion (ખોરાક ધીમેથી પચવો) can blunt your natural thirst signals. Ensure you drink a minimum of 2 to 3 liters of pure water daily. Adding clean electrolytes can help avoid the mild headaches often caused by early carbohydrate restriction.
Engage in Structured Resistance Exercise
Perform targeted strength or resistance exercise 2 to 3 times per week. This provides an essential structural signal to your body to retain lean skeletal muscle while focusing fat breakdown on stored adipose tissue.
9. Comparing Metrics: Type 2 Diabetes vs. Non-Diabetic Patients
Medical data shows a distinct variation in early weight loss progress based on your underlying baseline metabolic state. Patients utilizing Semaglutide who are also managing Type 2 Diabetes typically experience a more gradual weight drop during the initial weeks compared to non-diabetic individuals.
In standard study cohorts reviewed in accordance with the official FDA Clinical Product Label, non-diabetic subjects averaged a 6.3% reduction by week 12, while patients with Type 2 Diabetes averaged closer to 3.9%. This occurs because your biology prioritizes balancing blood sugar levels and repairing insulin issues before redirecting cellular energy to breaking down stored body fat.
10. Navigating Beyond Day 30: Progressing Your Maintenance Protocol
Completing your first 30 days marks the successful completion of your introductory phase. Following week four, your healthcare provider will guide your transition to the next step, escalating your weekly dosage to 0.5 mg once weekly. This continues your step-up progression toward standard maintenance settings.
To fully understand this long-term journey, read our detailed review on the comprehensive Semaglutide Weight Loss Timeline Guide to ensure your health outcomes remain steady over the next 6 months.
11. Comprehensive Frequently Asked Questions (FAQs)
Q1: Why am I not seeing major Semaglutide Before and After 30 Days Results yet?
A: It is a common clinical observation for patients to expect dramatic weight shifts within their first month of treatment. However, the initial 0.25 mg weekly dose is deliberately designed as an induction phase rather than a therapeutic fat-burning dose. The primary biological objective during these first 4 weeks is to prepare your gastrointestinal tract, upregulate your cellular GLP-1 receptor sensitivity, and safely accustom your enteric nervous system to a slower gastric emptying rate. Most clinical trial data demonstrates that notable, sustained reduction in adipose tissue typically begins once your clinical supervisor titrates your protocol up to higher therapeutic doses during the second and third months of consecutive treatment.
Q2: How much scale drop is normal for month one?
A: Peer-reviewed clinical research and real-world database outcomes published in the National Institutes of Health (NIH) STEP Program Registry indicate that a healthy, typical weight loss benchmark ranges between 2% and 4% of your total starting body mass over the initial 30 days. For an individual beginning their treatment journey at a baseline weight of 250 pounds, this translates mathematically to a safe drop of roughly 5 to 10 pounds. Losing weight at a gradual, steady pace of 1 to 2 pounds per week is highly recommended by medical experts to prevent systemic shock and preserve lean muscle fibers.
Q3: Does the initial 0.25 mg weekly dose suppress food cravings instantly?
A: Receptor response rates are highly individual and vary across different genetic profiles. Certain high-responding individuals notice a significant decrease in neurological “food noise” within the first 48 hours after their very first subcutaneous injection. Conversely, other patients with lower initial receptor density may require multiple weekly doses for the compound to reach a consistent, steady-state plasma level in their bloodstream. If your hunger suppression feels minimal during the first 30 days, do not be discouraged; your body is simply building the necessary molecular tolerance safely.
Q4: What food options optimize my first 4 weeks progress?
A: To maximize your early clinical results and avoid digestive issues, your daily nutritional plan must focus on dense, high-quality lean proteins alongside fibrous, low-glycemic carbohydrates. Because the medication creates slower digestion, eating highly processed items, deeply fried options, heavy creams, and simple sugars can trigger intense fermentation, bloating, and nausea. Center your daily meals around baked chicken breast, roasted turkey, egg whites, and cruciferous vegetables to support your body’s lean muscle tissues cleanly.
Q5: Can I bypass the starter dose to speed up my initial weight loss changes?
A: Skipping your initial titration schedule is strongly discouraged and poses serious medical risks. According to safety updates provided in the FDA Drug Label Database, attempting to inject a higher maintenance dose right away will overwhelm your digestive tract’s nervous pathways, frequently causing severe gastrointestinal distress. This sudden transition can result in persistent, uncontrollable vomiting, severe abdominal pain, and acute dehydration requiring hospital admission. Following a structured step-up schedule allows your body to safely develop metabolic tolerance over the long run.
Q6: How long do first-month digestive side effects last?
A: Minor gastrointestinal adjustments, such as mild intermittent nausea, temporary acid reflux, and early satiety shifts, generally peak during the first two weeks of initiating the 0.25 mg protocol. This occurs because the stomach is adapting to its new, slower rate of peristalsis. As your system reaches a stable concentration of the active peptide around weeks three and four, these symptoms usually fade or disappear entirely. Managing your portion sizes and eating slowly will significantly help keep your digestion comfortable throughout this transition.
Q7: Is fatigue standard when reviewing early monthly updates?
A: Experiencing mild fatigue or lower energy levels is a common report among patients during their first month of therapy. Data from the NIH/PubMed Trial Archives indicates this symptom is rarely a direct toxic reaction to the medication itself. Instead, it is usually a natural physiological adaptation to the sudden, steep reduction in your daily caloric intake. Because the reduction in cravings can lead to a rapid drop in carbohydrate consumption, your metabolism needs a few weeks to adjust to using stored body fat for fuel.
Q8: How can I protect lean muscle tissue during my first 30 days?
A: When your body experiences a sudden caloric deficit, it may naturally break down both stored body fat and active muscle tissue for energy. To protect your lean muscle structures and support a healthy metabolic rate, you must consume adequate daily protein, targeting roughly 0.8 to 1.2 grams per kilogram of body weight. Pairing a protein-conscious diet with structured resistance or strength training exercises 2 to 3 times a week signals your physiology to preserve valuable muscle tissue cleanly.
Q9: Is alcohol safe to consume during the first 30 days of treatment?
A: It is highly recommended to significantly limit or avoid alcohol consumption during your initial month on the medication. Alcohol can worsen common gastrointestinal side effects like nausea, acid reflux, and dehydration. Additionally, alcohol contains empty calories that can slow down your weight loss progress and may cause unpredictable drops in blood glucose levels, particularly for individuals managing underlying metabolic or insulin resistance issues.
Q10: What is the correct protocol if I forget an injection during month one?
A: If you miss a weekly injection, look closely at the timeline before taking action. As outlined in guidelines regarding FDA Unapproved vs Approved GLP-1 Usage Safety, if your next scheduled dose is more than 2 days (48 hours) away, go ahead and administer the missed injection right away, then resume your normal weekly schedule. However, if you are within 48 hours of your next planned dose, skip the missed one entirely and take your next regular injection on your usual day. Never inject a double dose to make up for a missed one.
Conclusion
Semaglutide represents a paradigm shift in American healthcare. By addressing the biological drivers of hunger and insulin resistance, it offers hope to millions struggling with Type 2 Diabetes and obesity. However, success requires a partnership with a medical professional and a commitment to whole-body health.
Disclaimer: This article is for informational purposes only and does not constitute medical advice. Always consult with a qualified healthcare provider before starting any new medication.